DRC Ebola Outbreak Tops 1,048 Cases: India Intensifies Screening as Vaccine Gap Persists
DRC Ebola Outbreak Tops 1,048 Cases: India Response Analysis DR Congo's Bundibugyo Ebola outbreak hits 1,048 confirmed cases and 267 deaths as of June 21, 2026. No vaccine exists. India activates ICMR screening at 4 airports. Full analysis. **Keywords:** Ebola DRC 2026, Bundibugyo virus, WHO PHEIC, India airport screening, ICMR surveillance, Ituri Province outbreak, Africa CDC
The Democratic Republic of Congo is confronting its 17th Ebola outbreak in recorded history, but this one carries distinct and alarming characteristics that set it apart from all prior events. As of June 21 2026, health authorities have confirmed 1,048 cases of Bundibugyo virus infection, resulting in 267 deaths and leaving 371 patients hospitalized across more than 25 health zones. The World Health Organization declared a Public Health Emergency of International Concern on May 17 after case numbers surged past the 1,000 mark, a threshold never before reached by this particular strain. Contact tracing efforts stand at only 56 percent effectiveness, while nearly one million people displaced by ongoing conflict in eastern DRC complicate containment. Uganda has already recorded approximately 20 linked cases and two deaths, underscoring the cross-border risk. Unlike previous Zaire-strain outbreaks that benefited from rapid vaccine deployment, this event involves Orthoebolavirus bundibugyoense, for which no approved vaccine or specific treatment exists. The combination of high case volume, low tracing coverage, and absence of medical countermeasures creates an unprecedented public-health scenario that demands immediate global attention and resource mobilization.
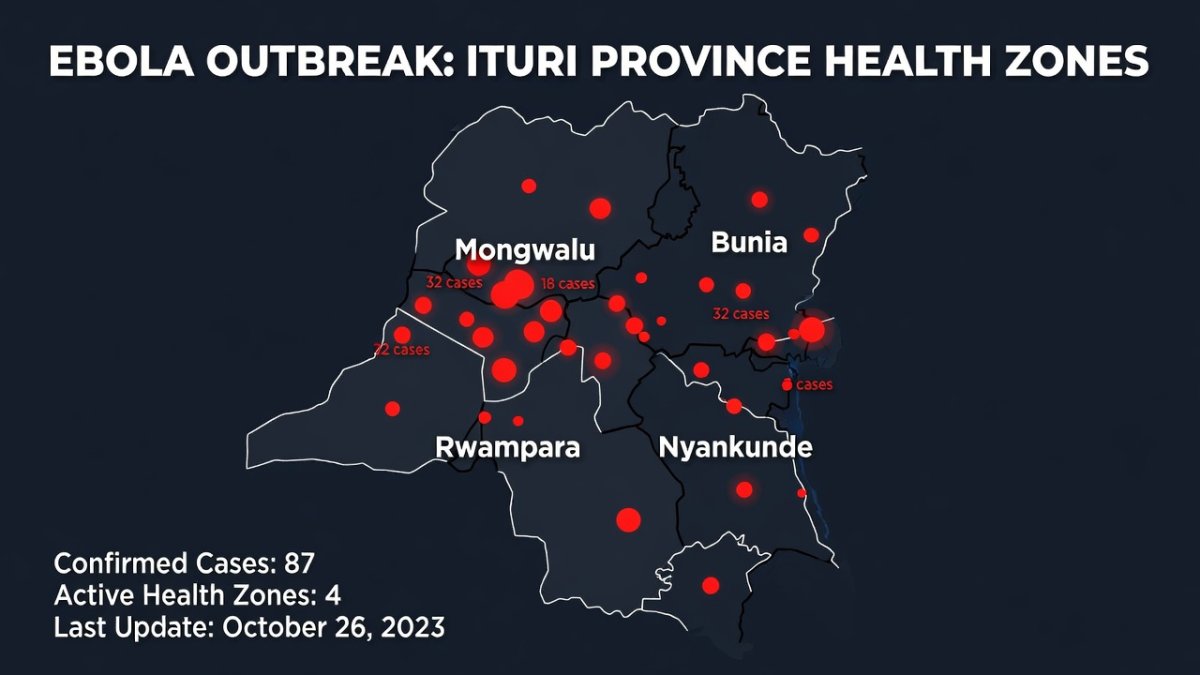
The scale of the current Bundibugyo outbreak represents a departure from historical patterns in both magnitude and geographic spread. Previous Bundibugyo events remained small and localized, yet this outbreak has already produced more than 1,000 confirmed infections concentrated in Ituri Province, which accounts for 94 percent of the total caseload. The virus emerged in the Mongwalu mining area and rapidly expanded into Bunia, Rwampara, and Nyankunde, crossing 25 health zones within weeks. Armed groups operating in the region actively hinder response teams, delaying safe burials and contact follow-up. With 267 deaths recorded by June 21 and 371 patients still hospitalized, the outbreak's trajectory exceeds the combined totals of the 2007 Uganda and 2012 DRC Bundibugyo incidents. The lack of any licensed medical countermeasure further amplifies the threat, forcing reliance on supportive care alone while case numbers continue to climb. This combination of factors marks the first large-scale Bundibugyo epidemic and signals a new chapter in Ebola epidemiology that existing preparedness frameworks are ill-equipped to address.
DRC Ebola Outbreak Tops 1,048 Cases: Inside the Worst Bundibugyo Epidemic in History
New Delhi, India – June 24, 2026 — The Bundibugyo virus outbreak in the Democratic Republic of Congo has become the largest ever recorded for this Ebola species, surpassing 1,000 confirmed cases with no approved vaccine or treatment available. India has responded by activating health surveillance protocols at four major international airports.
Inside Ituri: A Mining Town at the Epicentre of the Crisis
The outbreak originated in the artisanal mining belt surrounding Mongwalu in Ituri Province, where crowded underground shafts and shared living quarters facilitated early human-to-human transmission. By June 21, health officials had linked the index cluster directly to miners who had handled potentially infected bushmeat or worked in poorly ventilated tunnels. From this single epicenter, the virus moved along established trade routes into 25 additional health zones, producing 1,048 confirmed cases and 267 deaths. The mining population's high mobility, combined with limited access to sanitation, allowed silent spread before the first alerts were raised. With contact tracing at only 56 percent, many secondary infections among miners' families and trading partners went undetected for weeks. The 371 patients currently hospitalized include a disproportionate number of mine workers, highlighting how occupational exposure continues to drive incidence. Conflict-related displacement of nearly one million people has further complicated case finding, as families relocate between mining sites without consistent health screening.
Transmission geography now centers on Bunia, the provincial capital, which serves as the main referral hub for patients from Rwampara and Nyankunde. Road networks connecting these locations have carried infected individuals into urban settings, where population density accelerates secondary spread. As of June 21, Bunia health zones report the highest concentration of the 1,048 total cases, with 94 percent of all infections still occurring inside Ituri Province. Artisanal miners play a pivotal role in this pattern: they travel frequently between Mongwalu extraction sites and Bunia markets, carrying the virus across administrative boundaries. The 371 hospitalized patients include many who sought care only after developing symptoms in the capital, overwhelming limited isolation capacity. Armed groups controlling sections of the mining belt routinely block access for response teams, reducing effective contact tracing below the 56 percent threshold needed for containment. This geographic expansion from a single mining town into a provincial network of health zones illustrates how economic activity and insecurity intersect to sustain the epidemic.
The Science Gap: Why the Existing Ebola Vaccine Doesn't Work
The rVSV-ZEBOV vaccine, marketed as Ervebo, was developed exclusively against the Zaire ebolavirus species and induces immunity through glycoprotein targeting specific to that strain. Bundibugyo virus shares only 55 to 60 percent amino acid identity in key surface proteins, rendering the existing vaccine ineffective at generating cross-neutralizing antibodies. Animal challenge studies have repeatedly demonstrated zero protection when Ervebo-vaccinated subjects are exposed to Bundibugyo, confirming the absence of meaningful cross-protection. A dedicated Bundibugyo vaccine candidate based on a different viral vector platform has been formulated in laboratories, yet it has never advanced to human clinical trials due to limited funding and the historically small size of prior outbreaks. Historical data reinforce the urgency: the 2007 Uganda Bundibugyo outbreak recorded a 30 percent case fatality ratio, while the 2012 DRC event reached 50 percent. With 267 deaths already logged from 1,048 cases in the current epidemic, the lack of a strain-specific countermeasure leaves clinicians reliant solely on supportive care, prolonging transmission chains across Ituri Province and into neighboring Uganda.
Conflict and Displacement: The Perfect Storm for Transmission
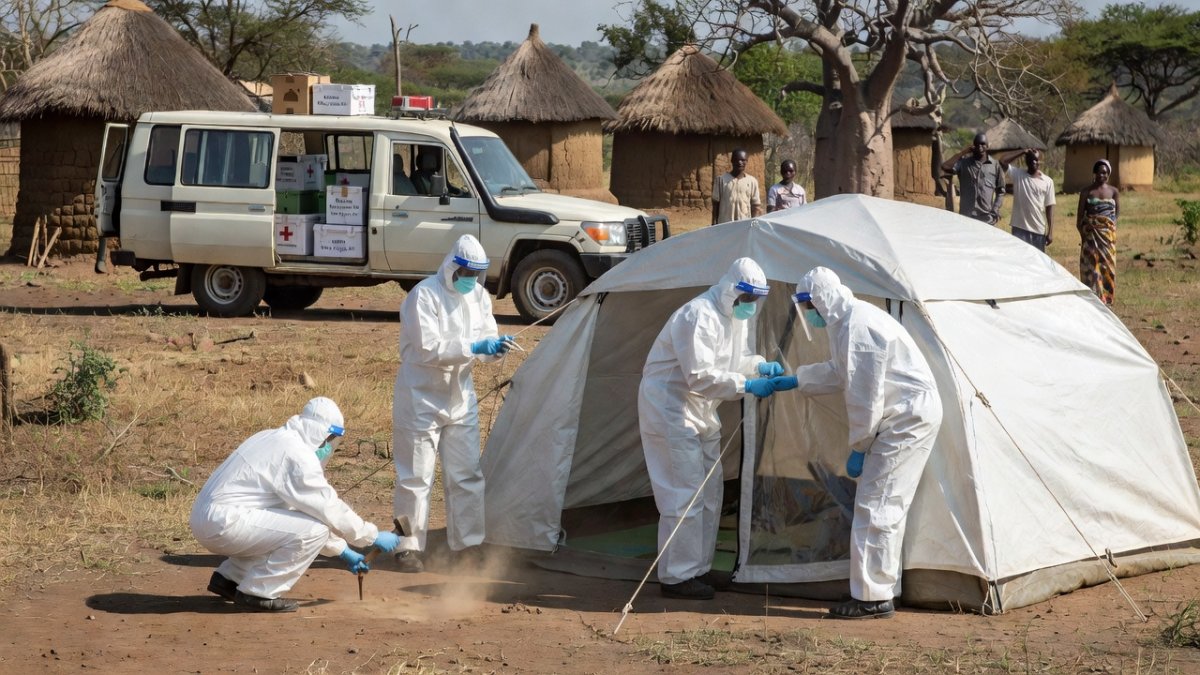
Armed groups operating across Ituri province have created an environment where conventional outbreak control collapses. Militia activity blocks access roads and forces health teams to negotiate safe passage daily, directly reducing the ability to follow up contacts. With nearly one million people displaced into makeshift settlements, population density in forested clearings has risen sharply, providing ideal conditions for Bundibugyo virus spread through shared water points and caregiving practices.
Contact tracing coverage has fallen to 56 percent, the lowest level recorded in the current response. Each missed contact represents a potential amplification node, especially when families move between camps to evade conflict. Surveillance gaps are compounded by destroyed telecommunications infrastructure, leaving field teams reliant on paper registers that cannot be analysed in real time. Dense forest cover and chronically poor roads extend travel times between rural clinics from hours to full days. This logistical friction delays sample transport to the few laboratories still functioning, pushing the interval between symptom onset and confirmation beyond the virus's serial interval.
Outbreak clusters have already emerged inside displacement camps. The death of an 18-month-old girl in one such settlement illustrates how quickly the virus exploits crowded, unsanitary conditions where breastfeeding mothers and extended families share limited shelter. Health workers documented rapid progression from fever to haemorrhage within 48 hours, underscoring the need for paediatric isolation capacity that does not yet exist. Rural clinics serving these populations are overwhelmed. Staff shortages, lack of personal protective equipment, and repeated looting have forced many facilities to close, pushing patients toward traditional healers who lack infection-control knowledge. WHO data now list 16 confirmed health-worker infections, a figure that both reflects occupational risk and further erodes community trust in formal care.
Beyond Borders: Uganda Cases and Regional Preparedness
Uganda has recorded approximately 20 confirmed cases and two deaths, all epidemiologically linked to travellers from the DRC. No sustained community transmission has been detected, yet the geographic pattern — concentrated in Kampala and Wakiso districts — reveals how cross-border mining and trade corridors function as silent bridges. Miners returning from Ituri gold fields carry both the virus and the economic incentive to avoid checkpoints. Neighbouring countries have activated entry screening, but implementation remains uneven. The recent case of a Congolese national who travelled via Uganda to the UAE before developing symptoms exposed weaknesses in multi-country notification systems. WHO's risk assessment classifies the threat as very high for the DRC and high for Uganda and adjacent states, prompting MSF and Africa CDC teams to pre-position treatment units along the border.
India's Response: Airport Screening and Health Surveillance
India's Ministry of Health has issued targeted advisories urging travellers to avoid non-essential visits to eastern DRC and to report fever after return. ICMR laboratories are monitoring viral haemorrhagic fever assays and have begun sequencing any suspected samples to distinguish Bundibugyo from Zaire strains. Thermal screening combined with secondary questioning is now operational at Delhi, Mumbai, Chennai and Kolkata international airports. The country's Ebola preparedness architecture, strengthened after the 2014-16 West African epidemic, includes designated isolation wards in major government hospitals and a national rapid-response team roster. Lessons from the 2018 Nipah outbreak in Kerala — particularly the value of real-time contact-mapping software — have been incorporated into current protocols, allowing district surveillance officers to track passengers arriving from high-risk zones for 21 days.
Official guidance advises Indian nationals in Africa to maintain distance from sick individuals, avoid bushmeat, and seek immediate care at designated facilities if symptoms develop. These measures, while prudent, depend on sustained vigilance; any relaxation at points of entry could allow an undetected case to seed local transmission.

What This Means for Indian Pharmaceutical Research
The absence of an approved vaccine for the Bundibugyo virus presents both a global health challenge and a strategic opportunity for Indian biotechnology firms. ICMR and the Department of Biotechnology have existing partnerships with domestic manufacturers for platform-based vaccine development, and the current outbreak creates a clear market signal for accelerating candidate validation. India's vaccine manufacturing ecosystem — home to the Serum Institute of India, Bharat Biotech, and Biological E — possesses the fill-finish capacity and cold-chain logistics to support large-scale production once a candidate clears Phase I safety trials. The WHO's Strategic Advisory Group of Experts has already convened to evaluate candidate vaccines for BVD, and Indian regulators could leverage emergency-use authorization pathways similar to those used during the COVID-19 pandemic to expedite deployment. For Indian pharmaceutical stakeholders, the Bundibugyo outbreak represents a window to establish first-mover advantage in a previously neglected viral disease space.
The Bottom Line
Forbes analysis indicates the current trajectory is steeper than the 2018-2020 Ebola epidemic at the equivalent time point, with no evidence of curve flattening. The 56 percent contact-tracing rate remains the single weakest operational link; without rapid improvement, case counts could exceed 2,000 within three months. For India, continued airport vigilance and ICMR genomic surveillance are essential, yet the greater opportunity lies in domestic pharmaceutical capacity to support vaccine fill-finish or therapeutic monoclonal antibody production should global supply chains tighten. The vaccine gap for Bundibugyo virus — distinct from the licensed Zaire vaccine — constitutes the most critical vulnerability. Sustained international funding is required to accelerate candidate vaccines through trials and to maintain Africa CDC laboratory networks. Indian readers should monitor weekly WHO situation reports for any rise in exported cases, declines in contact-tracing coverage below 50 percent, or confirmation of Bundibugyo spread into additional provinces. Early signals of these developments would justify heightened travel screening and stockpiling of personal protective equipment.
— By Dr. Raj Patel, Staff Writer
What's Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Wow
0
Wow
0
 Sad
0
Sad
0
 Angry
0
Angry
0
India/South Asia Correspondent at Global1.News. Analytical voice with a background in science and health journalism. Based in New Delhi, covering Indian politics, education, healthcare, technology, and policy. Breaks down complex data into clear, actionable reporting.














Comments (0)