Ebola Bundibugyo Outbreak: Rare Strain Spreads Across DRC and Uganda
Ebola Bundibugyo Outbreak: Rare Strain Spreads Across DRC and Uganda Lead — set the scene. What is happening, where, why it matters The Ebola disease caused by the Bundibugyo virus has emerged as a significant public health threat in the Democratic Republic of the Congo and Uganda. First reported in May 2026, the outbreak has already produced hundreds of confirmed infections ac
Ebola Bundibugyo Outbreak: Rare Strain Spreads Across DRC and Uganda
Lead — set the scene. What is happening, where, why it matters
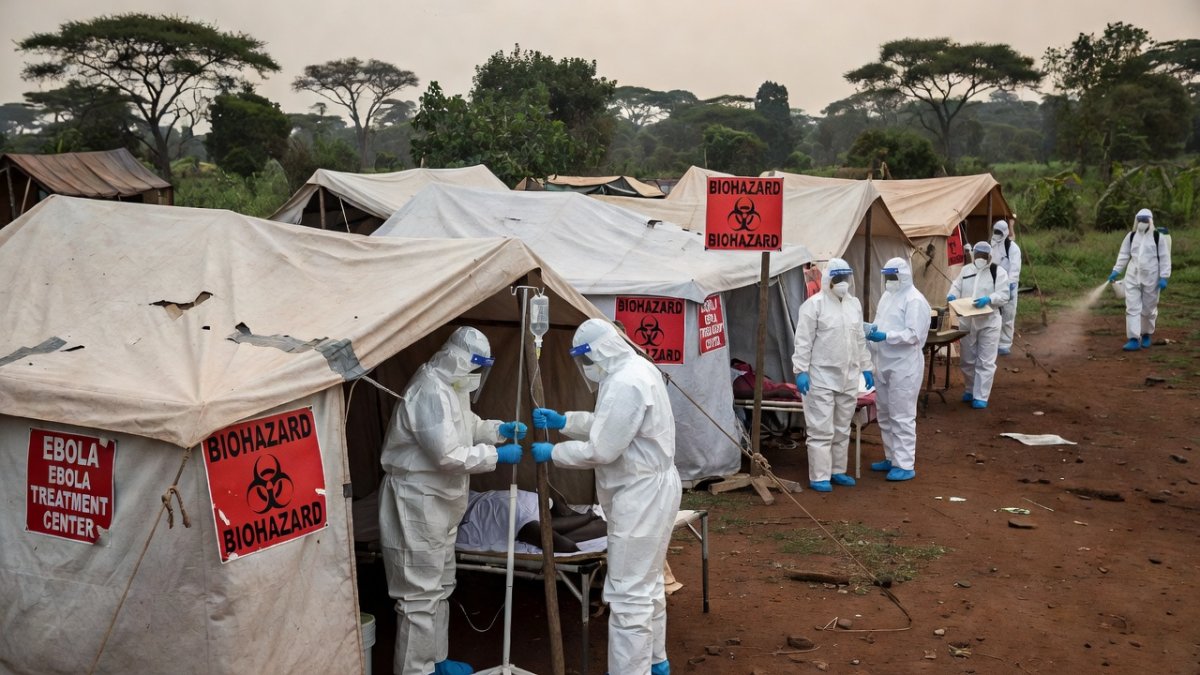
The Ebola disease caused by the Bundibugyo virus has emerged as a significant public health threat in the Democratic Republic of the Congo and Uganda. First reported in May 2026, the outbreak has already produced hundreds of confirmed infections across multiple provinces. Health authorities including the WHO have responded by declaring a Public Health Emergency of International Concern on May 17, 2026, underscoring the international implications of this rare strain.
DRC provinces including Ituri, Nord-Kivu, and Sud-Kivu report the bulk of activity, while Uganda has recorded limited but concerning spillover cases. The absence of approved vaccines or treatments specific to Bundibugyo virus distinguishes this event from prior Ebola responses. Existing vaccines targeting Zaire ebolavirus offer no protection, leaving populations vulnerable.
WHO data indicate 515 confirmed cases and 91 deaths in the DRC as of June 6, yielding a case fatality ratio of 17.7 percent. Uganda has documented 19 confirmed cases and two deaths through June 14. These figures, drawn from official surveillance, highlight the need for rapid containment measures coordinated by agencies such as the CDC and ECDC.
Regional aid organizations have warned that total cases may have surpassed 800 when unreported infections are considered, according to Bloomberg reporting on June 16. The situation matters because it represents only the third recorded Bundibugyo outbreak in history, following events in Uganda in 2007-08 and the DRC in 2012-13. International monitoring of travelers by the CDC and ECDC reflects the potential for further geographic expansion.
Dr. Lame of ALIMA noted that more options exist today and survival rates have improved compared with earlier outbreaks. Nevertheless, the lack of targeted medical countermeasures requires reliance on supportive care and strict infection prevention. The outbreak therefore tests the resilience of health systems already strained by other challenges in eastern Africa.
The outbreak's scale — numbers, locations, trajectory
Confirmed cases in the DRC stand at 515 with 91 deaths as of June 6, according to WHO figures. The provinces of Ituri, Nord-Kivu, and Sud-Kivu account for the majority of these infections. Uganda has reported 19 confirmed cases and two deaths through June 14. These numbers reflect laboratory-verified data compiled by national surveillance networks.
Bloomberg reported on June 16 that regional totals may have exceeded 800 when probable cases are included. Aid groups on the ground have cautioned that the trajectory could accelerate without intensified interventions. Historical context shows this remains only the third Bundibugyo event, with prior outbreaks limited to roughly 184 cases in Uganda during 2007-08 and 57 cases in the DRC during 2012-13.
Transmission patterns indicate sustained community spread in affected DRC provinces. Cross-border movement has already introduced the virus into Uganda, prompting enhanced screening at entry points. The CDC continues to track potential exported cases, while the ECDC monitors travelers returning from the region.
Projections from health agencies suggest that without accelerated contact tracing the case count could rise substantially in coming weeks. The current case fatality ratio of 17.7 percent in the DRC remains lower than some previous Ebola events, yet the absence of specific therapeutics limits clinical options. Trajectory modeling relies on timely reporting from field teams supported by organizations such as ALIMA.
Geographic expansion beyond initial hotspots remains a primary concern. Surveillance data indicate clusters in both rural and peri-urban areas, complicating containment. Continued monitoring by WHO and national authorities will determine whether the outbreak remains localized or develops into a broader regional event.
The cost of delay — the month before PHEIC declaration
The outbreak was first reported in May 2026, yet the WHO declaration of a Public Health Emergency of International Concern occurred on May 17. This interval of several weeks allowed undetected transmission chains to expand. Reports from WAMC/NPR have highlighted how the delay contributed to the subsequent growth in case numbers across DRC provinces.
Early signals of Bundibugyo virus circulation were not immediately escalated to international alert levels. By the time the PHEIC was issued, confirmed infections in the DRC had already reached several hundred. The resulting window permitted movement of exposed individuals across borders into Uganda before robust controls were established.
Retrospective analysis shows that earlier coordinated action might have limited the initial clusters. National authorities in the DRC faced logistical challenges in confirming the rare strain, which slowed the notification process. WHO guidance issued on May 28 regarding licensed vaccines came after the declaration and could not retroactively address the earlier spread.
The month-long period before formal emergency status also affected resource mobilization. Field teams required additional time to scale surveillance and laboratory capacity. UN News noted that Uganda’s subsequent response benefited from lessons learned, yet the initial delay had already seeded cases in neighboring territory.
Health officials acknowledge that faster recognition of the Bundibugyo strain would have enabled earlier deployment of emergency teams. The experience underscores the importance of rapid diagnostics for non-Zaire strains. Current efforts focus on compensating for the lost time through intensified cross-border coordination.
Why Bundibugyo is different — no vaccine, no treatment
No approved vaccine or specific treatment exists for the Bundibugyo virus. This distinguishes the current outbreak from those caused by Zaire ebolavirus, for which vaccines and therapeutics have been deployed. Existing Ebola vaccines target only the Zaire strain and provide no protection against Bundibugyo, leaving populations without immunologic defense.
WHO issued emergency guidance on licensed vaccines on May 28, yet these products remain ineffective here. Clinical management therefore relies entirely on supportive care, isolation, and infection prevention measures. The CDC and ECDC have emphasized the need for experimental approaches while acknowledging the absence of proven options.
Scientists are racing to test experimental therapies, as reported by the New York Times. These efforts include investigational antivirals and monoclonal antibodies originally developed for other Ebola species. Early data suggest some candidates may offer cross-protection, but rigorous trials are still required.
The lack of medical countermeasures increases dependence on non-pharmaceutical interventions. Contact tracing, safe burial practices, and community engagement form the core of the response. ALIMA teams have noted that survival rates have improved with better supportive care, yet the overall risk profile remains elevated due to the missing tools.
Research priorities now include accelerated development of Bundibugyo-specific vaccines. Regulatory pathways established during previous outbreaks may shorten timelines, but production and distribution will require substantial investment. Until such products are available, health systems must operate without the preventive shield used in Zaire outbreaks.
Cross-border spread — DRC to Uganda
The virus has crossed from the DRC into Uganda, producing 19 confirmed cases and two deaths as of June 14. Movement of people between the two countries facilitated this spillover. Surveillance at border points has since been strengthened to detect additional introductions.
Uganda’s health authorities activated emergency teams and laboratory networks immediately after the first imported cases. UN News commended these measures, which included rapid contact tracing and isolation of suspected patients. The response limited further amplification within Ugandan territory.
ECDC monitoring of travelers returning from the region supports early detection of potential exported cases. The CDC maintains similar tracking for international passengers. These systems aim to prevent additional cross-border seeding beyond the current DRC-Uganda corridor.
Geographic proximity of affected DRC provinces to the Ugandan border created multiple opportunities for transmission. Informal trade routes and family connections have historically enabled such movement. Enhanced screening and risk communication now target these pathways.
Continued vigilance remains essential because the outbreak in the DRC continues to generate new infections. Any relaxation of border measures could allow renewed spillover. Coordinated reporting between the two countries supports real-time adjustment of control strategies.
Conflict and contagion — M23 impact on response
The M23 rebellion in eastern DRC has complicated health operations in Nord-Kivu and surrounding provinces. Security constraints limit access for contact tracing teams and supply deliveries. Health facilities in contested areas face disruptions that hinder case detection and isolation.
Despite these challenges, response organizations continue to operate where possible. ALIMA and other partners coordinate with local actors to maintain surveillance in safer zones. The conflict environment increases the risk that cases remain undetected for longer periods.
WHO and national authorities have adapted strategies to account for insecurity. Mobile teams and community health workers provide coverage in areas where fixed facilities cannot function reliably. These adaptations have helped sustain reporting despite ongoing instability.
The rebellion also affects population movement, potentially accelerating virus spread along displacement routes. Aid groups monitor these dynamics to anticipate new clusters. Coordination with security actors remains necessary to protect health personnel.
Longer-term resolution of the conflict would facilitate more comprehensive outbreak control. In the interim, flexible operational models allow incremental progress. The combination of armed conflict and infectious disease creates a particularly difficult operational environment for responders.
What's being done — WHO, scientists, health workers on the ground
WHO has issued emergency guidance and coordinates international support for the affected countries. Surveillance networks have been expanded, and laboratory confirmation capacity strengthened in both the DRC and Uganda. These measures build on lessons from prior Ebola events.
Scientists are actively testing experimental therapies, as noted by the New York Times. Clinical trials seek to identify agents that may provide benefit against Bundibugyo virus despite the lack of approved options. Data from these studies will inform future treatment protocols.
Health workers deployed by ALIMA and partner organizations deliver supportive care and conduct contact tracing under difficult conditions. Dr. Lame emphasized that more people survive today due to improved clinical practices. Training and protective equipment help maintain staff safety during these efforts.
The CDC and ECDC provide technical assistance and monitor international travel. Their contributions include risk assessments and guidance for frontline responders. Collaboration across agencies ensures consistent messaging and resource allocation.
Community engagement forms a central component of current activities. Local leaders help promote safe practices and encourage early care-seeking. These ground-level actions complement higher-level coordination by WHO and national ministries.
Analysis and what happens next
The Bundibugyo outbreak demonstrates the persistent vulnerability created by the absence of strain-specific vaccines and treatments. With 515 confirmed DRC cases and additional infections in Uganda, the trajectory depends on sustained intensity of response measures. Historical precedents suggest that focused interventions can interrupt transmission when applied consistently.
Future progress requires accelerated research into Bundibugyo countermeasures. Regulatory and funding mechanisms developed for Zaire ebolavirus can be adapted, yet timelines remain uncertain. In the near term, reliance on supportive care and infection control will continue.
Cross-border coordination between the DRC and Uganda must remain robust. Any weakening of surveillance could permit renewed spread. International agencies including WHO, CDC, and ECDC will continue monitoring and providing technical support.
Security conditions in eastern DRC will influence operational reach. Improved access would enable more complete case finding and containment. Until then, adaptive strategies will determine the extent of further geographic expansion.
Overall, the evidence indicates that while the outbreak presents serious challenges, available tools and experienced responders offer a pathway toward control. Continued data collection and transparent reporting will guide adjustments. The coming weeks will reveal whether current efforts can reverse the upward trend in cases.
By Jessica Ali, Staff Writer
What's Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Wow
0
Wow
0
 Sad
0
Sad
0
 Angry
0
Angry
0
Editor-in-Chief at Global1.News. Atlanta-based journalist who cuts through the BS and tells it like it is. Lead anchor, host, and the voice you hear when the spin stops and the truth starts.














Comments (0)